Chiamata ai governi europei
MANIFESTO
10 risoluzioni per una nuova strategia di test su strisce di carta
[ EN ] -
[ FR ] -
[ DE ] -
[ NL ] -
[ IT ] -
[ ES ]
Chiamata ai governi europei
10 risoluzioni per una nuova strategia di test su strisce di carta
La ricerca mostra - e su questo punto c'è un consenso scientifico generale - che i moderni test di screening antigenici a basso costo possono aiutare efficacemente a rilevare i "casi corona" infettivi; e che i risultati migliori (e più affidabili) si ottengono quando questi test rapidi vengono applicati molto regolarmente (ad esempio giornalmente). Se utilizzato con sufficiente frequenza da alcuni gruppi di popolazione, può anche essere possibile ridurre il numero di casi di malattia da COVID-19 in Europa a quasi 0 ('close to zero'), perché alcuni membri dei gruppi statisticamente più rilevanti (a rischio) che sono stati recentemente infettati e che dovrebbero quindi essere identificati come potenziali spargitori di virus asintomatici, scopriranno immediatamente, tramite test ad alta frequenza, che sono davvero contagiosi, prima di poter infettare chiunque altro. In questo modo, è molto meno probabile che il virus si diffonda nella società, mentre le risorse mediche, scientifiche e diagnostiche saranno liberate per combattere efficacemente la pandemia.
Pertanto, questo tipo di 'screening della popolazione' massivo e il cosiddetto metodo di 'sorveglianza della salute pubblica COVID-19' ('COVID-19 public health surveillance') che ne è alla base, non solo protegge gli interessi privati di ogni singolo utente di autotest, ma anche - in primo - protegge il nostro interesse comune; a cominciare dalla salute pubblica di tutti gli europei.
È tuttavia prevedibile che il nuovo regime di screening come quello qui sostenuto (basato sui test della saliva su strisce di carta) dovrà - purtroppo ma necessariamente - essere mantenuto almeno fino al 2023; cioè, fino a quando il virus SARS-CoV-2 è mutato positivamente e ha diminuito sufficientemente la sua potenza di COVID-19 (cosa improbabile), o fino a quando che agenti antivirali (o modificanti la malattia) sufficientemente efficaci e/o vaccini protettivi (neutralizzanti o non neutralizzanti, ma comunque abbastanza durevoli) sarebbero immessi sul mercato (il che potrebbe essere possibile - - al più presto entro il 2023), o fino al raggiungimento dell'immunità di gruppo (minima) dopo che una coorte sufficientemente ampia è stata vaccinata con un vaccino immunosterilante efficace contro l'infezione da SARS-CoV-2 (che - entro il 2023 al più presto - è anche possibile).
Inoltre, tali aspettative devono essere confrontate e contrastate con gli obiettivi di alcuni vaccini di emergenza puramente 'COVID-19 protettivi contro la malattia' ('COVID-19 disease-protective') che sono ora in fase di sviluppo accelerato (alla fine del 2020), ma che purtroppo non offriranno una protezione permanente (o sufficiente) contro i rischi di infezione virale da SARS-CoV-2, che sono uno dei tratti distintivi di questo virus e che rendono questo virus e questa pandemia particolarmente pericolosi. A maggior ragione perché i suddetti vaccini d'emergenza (programmati al più presto per il 2021) offrono una prospettiva - in ogni caso - incerta, anche se gli obiettivi e le aspettative dichiarati - in ogni caso - sono per livelli di efficacia molto limitati, ufficialmente: "la prevenzione o mitigazione della MALATTIA, NON DELL'INFEZIONE" ("the prevention or mitigation of DISEASE, NOT INFECTION"), che in termini di efficace controllo della malattia da COVID-19 - secondo gli obiettivi ufficiali dei produttori - ammonta a una protezione di circa il 50% a 70% (e anche allora: solo parziale) contro alcuni importanti sintomi della malattia COVID-19.
In altre parole, e quindi non ci sono malintesi su questo tema: anche se presto saranno ampiamente utilizzati gli autotest rapidi qui consigliati, i "progressi medici fondamentali" tanto attesi dall'opinione pubblica europea nel campo della protezione contro il rischio di trasmissione di SARS-CoV-2 e/o nel campo dei metodi di trattamento per COVID-19, sono - allo stato attuale delle cose, anche secondo le previsioni più ottimistiche - attesi solo nel 2022-2023. Ecco perché - in ogni caso - rimarrà sempre necessario, in coerenza con la strategia iniziale di 'appiattimento della curva' ('flatten the curve') e di 'mitigazione dell'infezione' ('infection-mitigation'), mantenere molte delle attuali politiche di prevenzione, al fine di ridurre prima il numero di infezioni da SARS-CoV-2 - a tutti i costi - e in seguito di mitigarle il più possibile.


E fare questo: senza prescrizione medica, sulla base di semplici test antigenici della saliva su striscia di carta che danno un risultato sufficientemente affidabile entro 15 minuti (come altri "autotest di riferimento", come i classici test do-it-at-home delle urine HCG di gravidanza).
In altre parole: cambiare completamente rotta e implementare un regime di screening-test completamente nuovo, massiccio e decentralizzato. Distribuire alla popolazione enormi quantità di test della saliva, che da un lato possono essere effettuati in modo massiccio e rapido, senza alcun intervento medico, e senza alcuna necessità immediata di ricorrere ad apparecchiature o dispositivi di laboratorio specializzati, ma che dall'altro dimostrano in modo affidabile la negatività del virus, e quindi si trasformano in un 'VIRUS POSITIVO = NON OK! o 'NO GO' o 'NOT OK' se l'utente è già contagioso o minaccia di esserlo (o in un'altra situazione piuttosto eccezionale in caso di test poco frequenti: se l'utente può essere stato contagioso ma presto non lo sarà più, cosa che può essere facilmente verificata con un nuovo test qualche ora dopo).
(1) Autoisolamento immediato, fino a prova contraria.
(2) Un test "di conferma" istantaneo della saliva su striscia di carta (cioè un test di conferma basato su una diversa composizione molecolare, o anche su una tecnologia Ab monoclonale leggermente diversa).
(3) Auto-tracciamento dei contatti recenti dell'utente dall'ultimo test della saliva.
(4) Eventualmente/Facoltativamente un ulteriore test diagnostico clinico "di conferma" (RT-PCR).
In particolare fare appello al buon senso e allo spirito civico degli utenti che effettuano questi test salivari nella sfera privata del proprio domicilio, senza alcun obbligo di comunicare i risultati alle autorità competenti.
Per importanti eccezioni a quest'ultimo principio, vedere la seguente Risoluzione n. 04.

A seconda delle circostanze concrete, e solo per quanto strettamente necessario, tali risultati di "screening organizzati" possono essere soggetti a misure individuali o collettive, dirette e coercitive (come, ad esempio, l'isolamento o la quarantena), ma solo a condizione che sia rispettata la privacy di ogni individuo, compresi alcuni diritti sociali di base, il diritto del lavoro e altri diritti umani personali e/o collettivi.
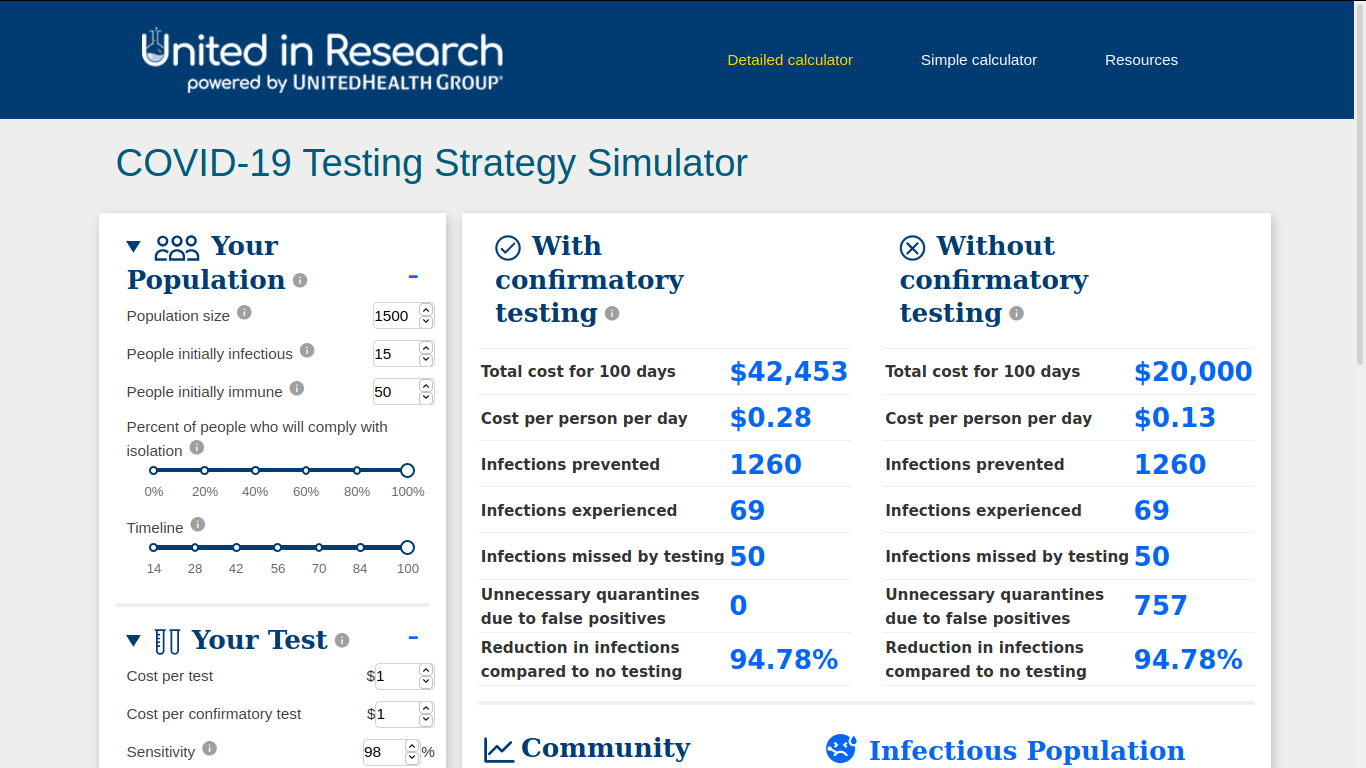
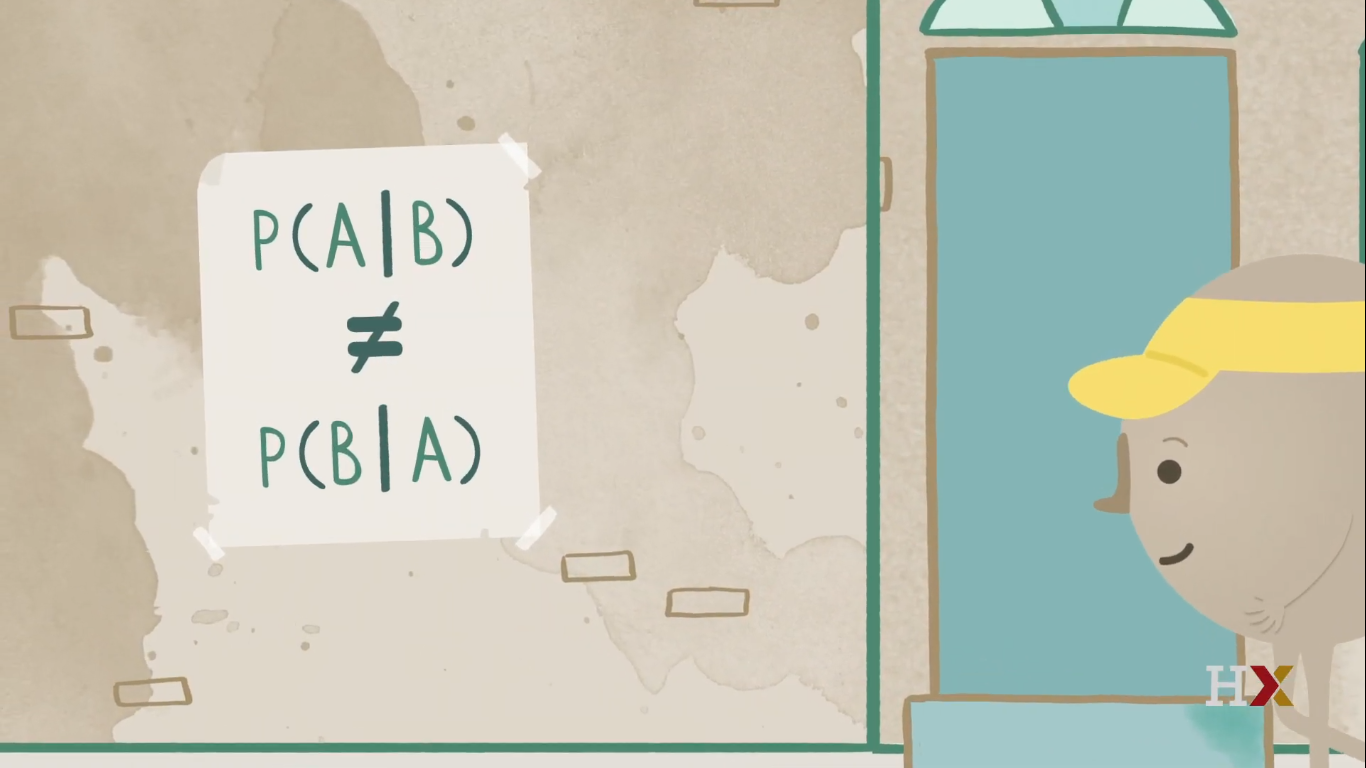
Come misura di sicurezza, nel contesto dei "test salivari organizzati", fornire ad alcuni di questi organismi una serie di test della saliva "di conferma" molecolarmente diversi, che possono servire come doppio test di conferma, ad esempio nel caso in cui uno degli studenti, degli insegnanti, del personale, della facoltà o degli altri membri risultasse positivo, o nel caso in cui un gran numero di test rapidi della saliva producesse inspiegabilmente un numero insolitamente "anomalo" di risultati positivi o negativi. In effetti, la probabilità di risultati "falsi positivi" può di solito essere significativamente ridotta da tali test di "conferma" (doppia conferma). E nel tentativo di aumentare drasticamente il controllo di qualità e in vista di un'abbondante vigilanza da parte degli "organismi organizzatori" che organizzano e/o coordinano ampi programmi di screening, l'uso di "test di validazione" può anche ridurre significativamente il rischio di risultati "falsi negativi" e/o " falsi positivi" (ad esempio implementando campioni di convalida "intelligenti"). Pertanto, gli enti organizzatori più evidenti dovrebbero essere sufficientemente avvertiti e informati sull'impatto statistico di concetti quali "prevalenza", "sensibilità" e "specificità" sulla probabilità di risultati "falsi positivi" e dovrebbero ricevere informazioni sufficienti su come controllare ed elaborare al meglio i risultati dei loro test di gruppo.
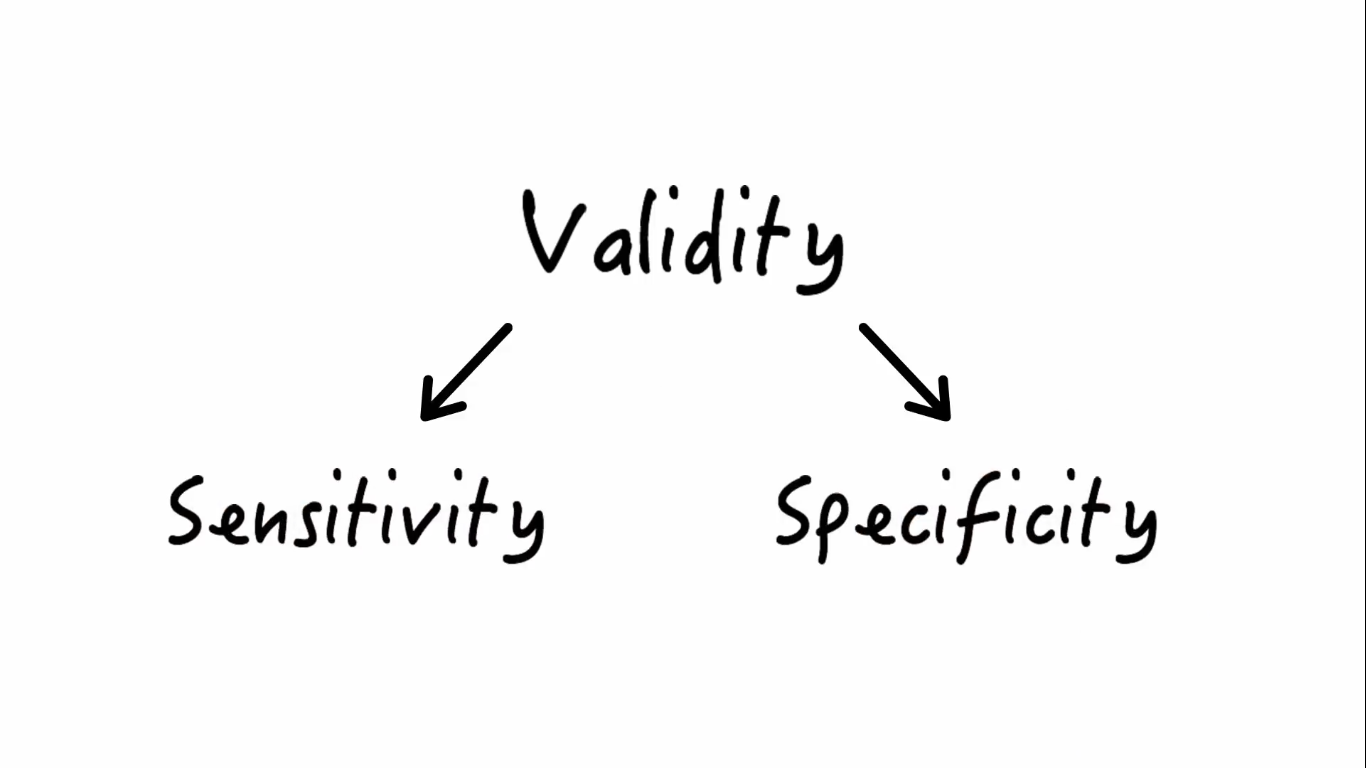
● Gli autotest sulla saliva su striscia di carta sono relativamente meno accurati: - Paper strip saliva self-tests are relatively less accurate: after all, they are slightly less sensitive and slightly less specific; which can have several consequences.
On the one hand, this can give rise to a greater probability of 'false positive' results,
which can subsequently be compensated for by an almost identical confirmatory saliva test (albeit with a different molecular composition), or by a classic RT-PCR test, or otherwise by simply repeating the same saliva test a few hours later.
On the other hand, there is a limited risk of "false negative" test results - during a short period of a number of hours at the very beginning of the traditional Corona "infectivity peak", which in most cases tends to be asymptomatic; but this limited risk is in turn - certainly if considered across the entire population - offset by factors such as the following:
a) an anyhow relatively low individual "viral load" at the start of infectiousness/transmissibility;
b) a high probability of being 'caught' or 'discovered' in subsequent tests, given the typically-high (e.g. daily) test rate for a representative user of paper-strip self-tests;
c) fast response times in case of the self-tests in comparison with the long turnaround times for highly specific and / or highly sensitive diagnostics where, instead of the hereproposed 15 minutes, the test results will take at least 6 to 24 hours and (all too) often even up to several days, leading to an increase of the actual risk of infection run by a 'positive' patient upon using high-quality albeit 'slow' 'test methods such as RT-PCR laboratory diagnostics, that may eventually turn out to be considerably riskier than in case the same test person - ceteris paribus - would have used a screening method based on the 'rapid' do-it-yourself saliva tests;
d) As a result of the massive deployment of the intended paper-strip saliva tests, many infectious virus carriers are indeed removed from the cohort (ie from the general population), and particularly at those very moments when they are the most contagious (ie during their SARS-CoV-2 infectiousness/trasmissibility peak).
● Gli autotest della saliva su striscia di carta sono notevolmente più efficaci: - Paper strip saliva self-tests are considerably more effective: they are much easier to use (at home or outside), and they also provide their users with the intended 'GO - NO GO' test results much faster. This is particularly important when symptomatic or asymptotic Corona virus carriers are going through their viral peak (a period of approximately 60 to 72 hours, with the highest viral load and viral shedding, so with the highest transmissibility, i.e. with the highest risk of infection).
● Gli autotest della saliva su striscia di carta sono notevolmente più economici (fattore 1/100): - Paper strip saliva self-tests are considerably cheaper (factor 1/100): after all, they consist (in principle) only of a paper strip test without further medical intervention. Since they are not capital-, labor- or time-intensive (and - at a rate of € 1 per test - are much more cost-effective), antigen saliva paper-strip tests make it possible to test on an individual basis much more frequently: for example daily, or on working days or school days, or prior to boarding an airplane, a bus or a taxi, or for example at very frequent, regular times: every 8, 12, 24 or 48 hours, etc.).
● Gli autotest della saliva su striscia di carta sono estremamente "scalabili" (estensibili): - Paper-strip saliva self-tests are massively 'scalable': unlike other means of testing they can be quickly and easily produced on a massive scale, almost without limits, as they consist of relatively simple paper-strips that are relatively easy to manufacture in specialized printing and packaging factories. Given the ultra-light nature of these strips, their distribution will also be lowcost and predominantly problem-free.







In ogni caso, fornire sufficienti "test di conferma" (si tratta di test della saliva quasi identici, che differiscono leggermente a livello molecolare dai test standard e possono quindi determinare in modo affidabile se l'utente si trova o meno di fronte ad un risultato "falso positivo").
Ad esempio, con ogni consegna di 100 test standard, i produttori potrebbero includere almeno 10-15 test aggiuntivi di conferma.
Le offerte, le specifiche, i termini di riferimento e i moduli d'ordine che vengono redatti al momento dell'acquisto dovrebbero prevedere una tale disposizione, in quanto questo sistema di conferma del "secondo parere" potrebbe rivelarsi molto utile in seguito, al fine di evitare o risolvere tutta una serie di problemi (ad esempio un improvviso aumento del numero di tester "falsi positivi") e altri inconvenienti, insoddisfazione, mancanza di fiducia, ecc. che dovrebbero essere evitati.
Come per la distribuzione delle maschere corona, la distribuzione di 'rapid test' dovrebbe essere gratuita, così come la distribuzione gratuita di preservativi o la fornitura di test diagnostici gratuiti all'inizio dell'epidemia di HIV/AIDS a metà degli anni '80 - un virus per il quale non è stato ancora sviluppato un vaccino efficace (35 anni dopo).
Nota: anche se la pandemia di SARS-CoV-2 / COVID-19 in caso di infezione o malattia offre prospettive di sopravvivenza significativamente migliori rispetto alla corrispondente infezione o malattia all'inizio della pandemia di HIV/AIDS, il mantra dovrebbe sempre essere che la prevenzione è meglio della cura, quindi per il momento, la prevenzione delle infezioni virali da SARS-CoV-2/COVID-19 merita una priorità assoluta, rispetto alla ricerca di trattamenti o alla ricerca di vaccini COVID-19. Dopotutto, non si può semplicemente presumere che questa situazione di crisi del COVID-19 attualmente in corso sarà definitivamente risolta entro i prossimi 6 mesi.
Inoltre, c'è sempre più bisogno di una serie di attività umane senza maschere facciali: alcuni contatti sociali e familiari, educazione di gruppo, eventi sportivi e culturali, ecc. Tali attività possono essere svolte solo se vengono prese adeguate precauzioni e misure preventive.
Dare priorità ai "test frequenti e rapidi" è una parte essenziale di qualsiasi politica di prevenzione delle infezioni da corona, con l'obiettivo di isolare il maggior numero possibile di individui infetti, in modo che la vita normale possa continuare e affinché le nostre strutture sanitarie non rimangano "esponenzialmente" sepolte sotto una valanga di casi COVID-19 urgenti e ad alta intensità di cure. Il metodo di auto-screening della saliva, come qui raccomandato, è la strategia più efficace ed efficiente (se non l'unica estensibile, quindi praticabile) per rimuovere da tutti i tipi di strati sociali e demografici il maggior numero di casi infettivi, nel modo più rapido ed economico possibile - ovunque e in qualsiasi parte d'Europa; almeno fino a quando risulteranno di nuovo negativi e quindi non rappresenteranno più alcun pericolo per i loro concittadini europei.
La forza intrinseca di questo metodo di screening rapido risiede negli effetti bio-statistici ed epidemiologici di un auto-testing continuo, frequente e massiccio da parte dei singoli cittadini, che scopriranno immediatamente i risultati dei propri test. È quindi essenziale che i nostri concittadini europei ricevano un numero massiccio di test il più presto possibile, in modo che possano iniziare a eseguire i test istantanei in gran numero.






Repubblica-video-rrtv-650-covid_speranza_100mila_tamponi_a.png)
Markus Lanz vom 13.08.2020-qas8pE5N_iQ-qas8pE5N_iQ.png)

Base scientifica
Adattare la politica di screening alle più recenti conoscenze scientifiche. Garantire che la salute pubblica europea (e le conoscenze scientifiche in materia) abbia la precedenza sull'economia europea. Prendere la scienza sul serio: includendo l'economia della sanità pubblica, la governance della salute pubblica, la virologia, l'immunologia, l'epidemiologia e la bio-statistica.
Adottare le misure pubbliche necessarie per proteggere la salute pubblica europea, ma farlo nel modo logisticamente più ragionevole e statisticamente più efficiente; anche se si devono utilizzare mezzi di test meno accurati (sub 'Gold standard', sub-RT-PCR), come gli autotest rapidi antigenici.
Incoraggiare il dibattito scientifico, ma stabilire un rapido consenso scientifico sulle sfide politiche più urgenti che richiedono un controllo centrale e decisioni rapide (come i metodi di screening della popolazione basati sui test domiciliari antigenici). Comunicare su questo con una voce chiara.
Informare accuratamente le autorità politiche e sanitarie locali di tutte le decisioni prese a livello centrale, nonché delle basi scientifiche di tali decisioni.
Sussidiarietà
Fare a livello locale, ciò che meglio può essere organizzato e implementato a livello locale. Sostenere le autorità locali con le loro politiche.
Ma nel caso - come nel caso della pandemia di corona - che alcune autorità locali rischiano di perdere il controllo della situazione o che chiaramente non hanno una sufficiente padronanza della politica, non esitare a intervenire, coordinare e organizzare tale politica al loro posto (e, se necessario, ad anche attuare questa politica al loro posto) a un livello più alto e più centralizzato. Nel caso del metodo di screening dell'autotest a livello europeo: a livello della Commissione europea e/o a livello nazionale degli Stati membri.
Nel caso in cui questo minacci di degenerare in un qualsiasi tipo di dibattito politico, condurre queste discussioni nel rispetto della scienza e tenendo conto degli input politici e delle proposte avanzati dagli scienziati. Vale a dire, sottoporre il più possibile il processo decisionale politico al consenso scientifico "applicato" stabilito.
Politica di applicazione seria
Attuare una seria politica di applicazione nel contesto delle misure e dei mandati della corona; soprattutto nel campo delle maschere facciali corona e degli autotest corona. Informare accuratamente le autorità locali di tutte le decisioni prese a livello centrale e della base scientifica di tali decisioni. E informare i cittadini delle conseguenze mediche e scientifiche delle loro azioni, nonché delle possibili conseguenze legali di tali azioni; o di non compiere questi atti.
Ragionevolezza - Solidarietà
Nella misura in cui ci si può ragionevolmente aspettare dai cittadini europei, fare appello alla loro comprensione, alla loro solidarietà intergenerazionale, al loro buon senso e al loro senso morale del dovere civico.
Anti-Viral Therapeutics & Emergency Vaccines:
Raise awareness and inform the European citizens, and make clear to them that both A) the current development of antivirals, and B) the development / introduction of some new emergency vaccines, will not suffice in the short to medium term to put an end to the high (exponential) risk of infection that is typical for the SARS-CoV-2 virus. Make clear to the European population that the emergency vaccines that are currently being tested are (for the time being) only aimed at a very limited scope of COVID-19 disease control objectives, but that they will certainly not be sufficient to effectively reduce the acute interpersonal SARS-CoV-2 contamination risks (which, for example, emanate from pre- and asymptomatic SARS-CoV-2 virus carriers, and particularly from the infamous Corona-super-spreaders).
Hospital Treatment & Diagnostics:
Raise awareness and inform the European citizens, and make clear to them that the recent progress made in hospital treatment techniques will not suffice indeed, whereas the widespread use of traditional diagnostic testing techniques (such as RT-PCR) for purely technical-logistical reasons is simply not suitable to be expanded 50-fold, or to be transposed from the medical laboratories to the kitchen or to the bathroom, to the station, to the office or to the school campus; let alone that the time frame required for these diagnostic tests could easily be reduced to less than 15 minutes - let alone on the basis of a mere saliva sample. Nevermind the fact that the (overworked) services that run this overburdened RT-PCR test infrastructure, and which are under ever more pressure to reduce turnaround times for these testing platforms, are probably unable to guarantee the duefull protection of the privacy / anonymity of their patient data. Let alone that they could offer such privacy guarantees for the forseeable future. Incidentally, proposals are popping up all over Europe all the time that jeopardize the aforementioned anonymity / privacy of test user data.
Screening & Diagnostics:
Therefore, make clear to the European citizens that they should not be too hopefull or naive in the short to medium term.
The mere "testing, testing, testing" paradigm or the mere approval of an "emergency vaccine" (whatever its ultimate efficacy may be) or the mere introduction of "new treatment techniques" will certainly not suffice to exit the crisis in the short to medium term.
Test Regimen & Pandemic Strategy:
Therefore, make clear to European citizens that they will have to adapt - in any case - to the fact that the recent profound behavioral changes, as adapted since March 2020, will also be necessary in the medium term (i.e. well into 2021 and 2022). And that thus - despite the obstacles described hereabove - the competent authorities will have to switch to a number of alternative strategies and new methods to reduce the acute (often invisible, because asymptomatic) contamination risks that arise in the context of this COVID-19 pandemic as caused by the SARS-CoV-2 virus, in their ongoing effort to mitigate the pandemic.
The most important tool - in addition to the classic face mask - to help European citizens keep up with the expected behavioral change (s) and with this kind of drastic social restrictions, is a new self-test screening regime based on paper-strip saliva tests.
PROS / ADVANTAGES of the New Screening Test Regimen:
-
very fast test taking ~ carrying out a saliva test can be done very quickly, when appropriate or convenient (24h/7d)
'point of need' ~ carrying out the tests can be done wherever and whenever it is appropriate ~ unlike traditional (diagnostic) 'point of care' or laboratory tests
routine job ~ daily users can take this test on their own in less than 1 minute on a routine basis, to read the result of the test less than a quarter hour later
ready-to-use ~ new testing regime that can be immediately implemented ~ no need for new anti-viral drugs, no need for new medical treatment methods, no need for additional medically / para-medically trained personnel, no need to wait for the new 'emergency vaccines', no need for doctor visits or COVID-19 hospital admissions, no dire shortages of diagnostic test tube reagents, etc. ~ the necessary technology and infrastructure are already largely available
‘fast positives’ ~ virus positive cases get an almost instantaneous 'NO GO' or 'NOT OK' test result, and can adjust to this result immediately
rapid isolation ~ virus positive testers can go into isolation immediately within 15 minutes after the test is administered, with the possibility of an additional 'confirmatory' saliva test and / or a confirmation based on a gold standard clinical RT-PCR diagnosis
possibility of immediate counter-assessments ~ direct access to a confirmatory test ~ for confirmation purposes, a limited number of identical paper-strip saliva tests are also supplied with every 100 paper strips that work on the basis of an alternative molecular composition (= double-check)
"Fast negatives" ~ virus negative cases get the 'GO' or 'OK' result of their test very quickly, and can continue the activities that are planned for the rest of that day in an unhindered / unabated way; albeit - evidently - without prejudice to the continued observance of the applicable preventive precautions
user-friendly ~ test results are easy (and without risk of confusion or differences of interpretation) for laymen and users to read and to understand
safe ~ by definition the testing protocol involves self-testing ~ in other words, no assistance from third parties or specialized personnel is required, so that these third parties can never become infected during the taking of the test ~ unlike with PCR tests, no "Martians"/PPE are required, which in turn saves a lot of time and money
low cost ~ can be applied on a massive scale by the entire population (eg daily, at less than € 1 per test) ~ economic leverage effect ~ negative opportunity costs + return on investment
"scalable" ~ test that can be applied massively (= by the masses + frequently) in the short to medium term ~ ideal for pandemic screening and / or population screening ~ this is a very interesting feat not just for the users, but also for their organizations and authorities
statistically relevant ~ (structured) test results can assist scientists and policymakers in their decision-making ~ decentralized population screening = a cheap research, development and policy tool
practical / effective triage tool ~ interplay between screening and diagnostics ~ the new paper-strip saliva test screening method is an ideal supplement and / or precursor and / or selection and triage tool for traditional diagnostic tests, which addresses the massive demand / need for RT-PCR tests, whereas at present such massive numbers of RT-PCR-tests can absolutely not be handled by hospitals and diagnostic labs
anonymous ~ (in principle) no need for track & trace ~ protection of privacy ~ protection against 'big brother' and against so-called 'digital surveillance capitalism'
comfortable ~ can easily be taken at home by laymen - no need for terrifying nose swabs, no need for complex lab equipment
compact ~ is portable and stowable ~ can easily be carried in a pocket in a jacket or in a backpack or in a handbag
child-friendly ~ comfortable for children aged 7 to 77, and possibly for those who are younger or older
practical for traveling ~ eg public transportation, airplanes, etc.
practical for on the road ~ eg work, school, hospital, theater, station, airport, stadium, place of worship, workshop, Christmas party at grandma's, etc.
CONS of this new (less accurate) public screening rapid testing regimen:
-
limited risk of "false negatives" if the test is not administered correctly and / or if the test results are not correctly read and / or misinterpreted
~ However: all kinds of precautions can be taken by the user himself/herself (e.g. assistance of children and the elderly, 4-eyes principle within the same family, pointing-and-calling method, test in a quiet room such as a bathroom, etc.). Organizing organizations can also take extra precautions. And in the first place, the manufacturers themselves will of course take the best precautions - as much as possible and as useful as possible. In addition, the government and the media can also raise awareness among the population about the risks of 'false negatives', which will always exist anyway (as they do with other tests), and which of course should not be underestimated. ~ Past experience with other self-tests (such as pregnancy tests, HIV tests, etc.) shows that this type of risk does not have to be an insurmountable problem, and that in developed countries (such as the EU member states) these risks practically can be reduced to almost zero. But even then, even if something goes wrong now and then, the ultimate global effect of this screening method remains predominantly positive, and its ultimate impact remains much better than anything that has been tried so far.
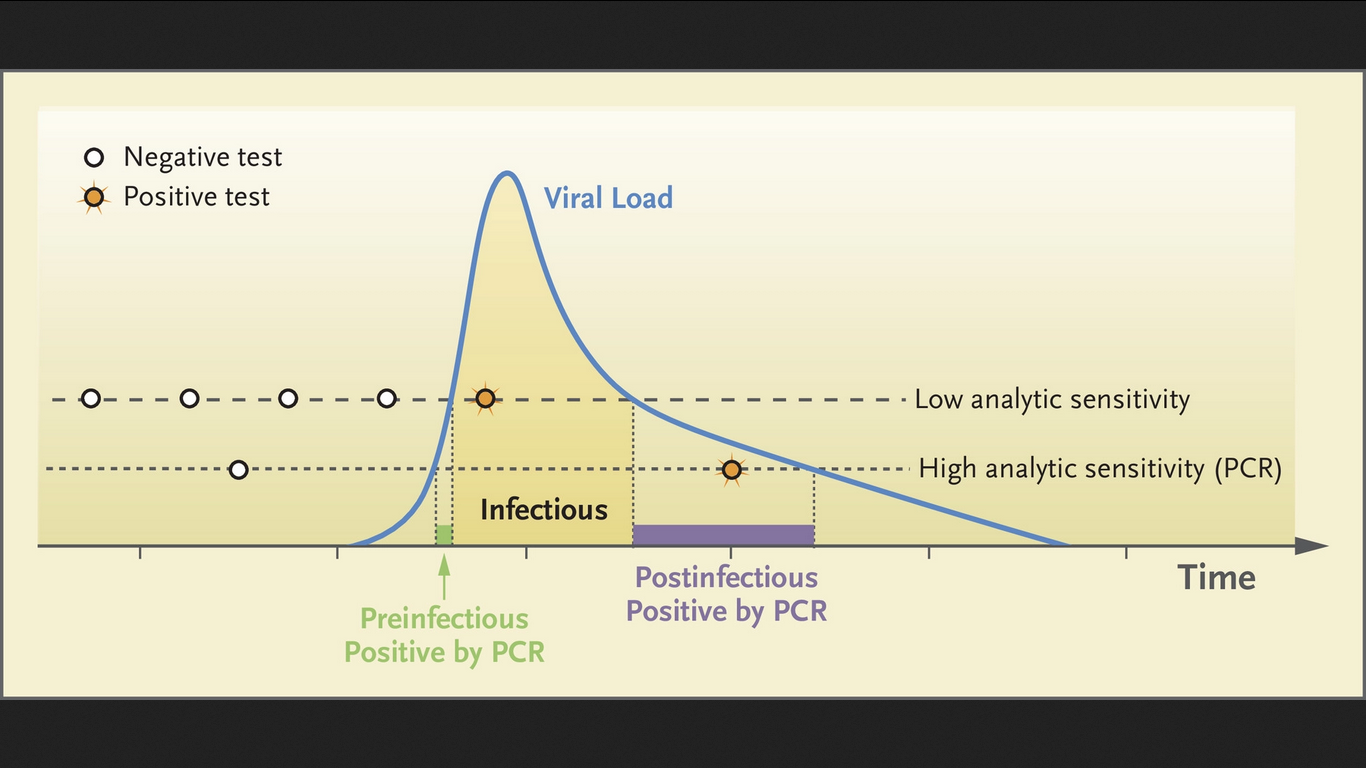
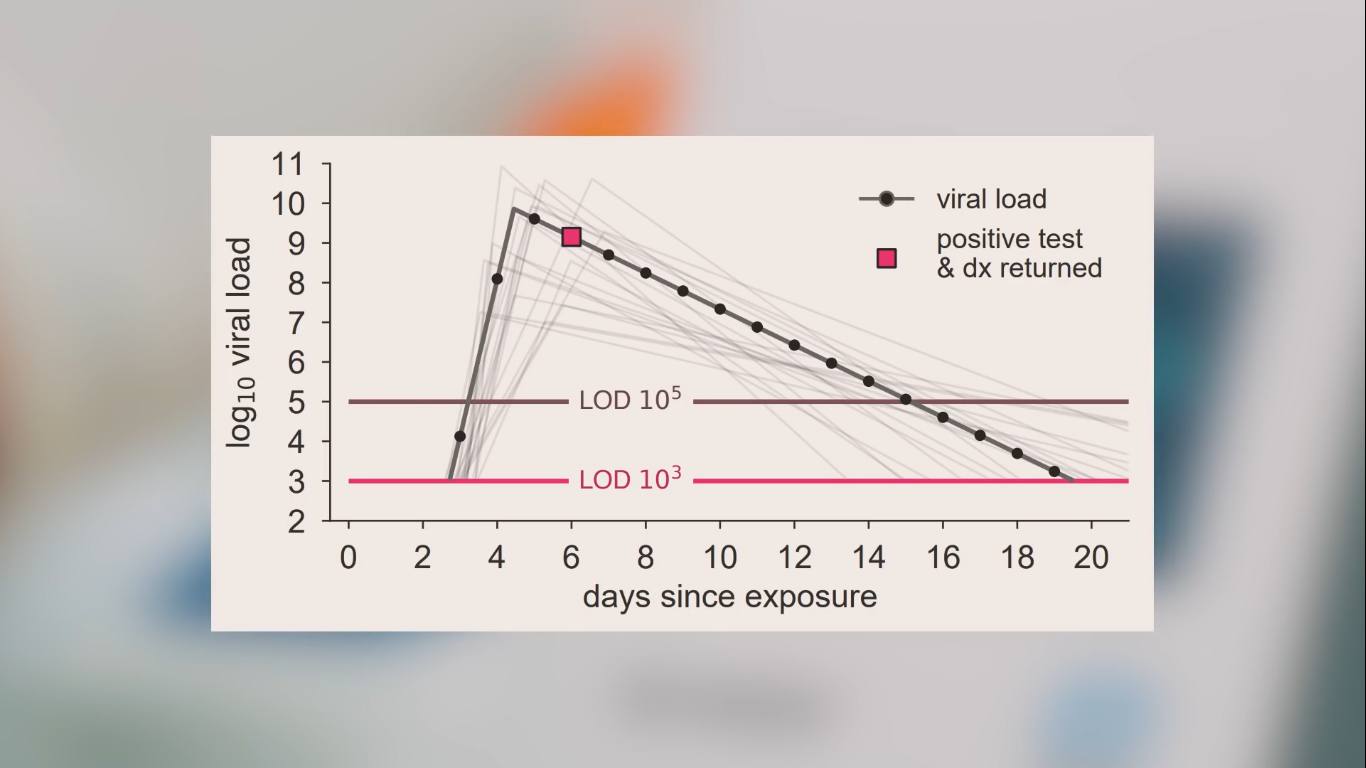
limited risk of 'false negatives' at the (in any case asymptomatic/presymptomatic) very beginning of the 'highly-virus-infectious phase'; this is the 'Virus Infectious / Transmissible Phase with high viral loads and high viral shedding' = 'Ultra-Ansteckende Phase'
~ However: during their so-called 'viral peak' (60-72h with highest risk of infection) this 'initial risk' for false negatives in virus-positive test users is not statistically relevant (thus negligible) from an epidemiological point of view; although it may be useful to remind each test user at an individual level of the existence of the (limited) probability of 'false negatives' at the very beginning of the virus-contagious phase: this risk is not to be 100% neglected indeed, so that other precautions must still be permanently observed.
likelihood of "false positives" (especially given certain typical Bayesian effects), which may give rise to an increasing demand for additional RT-PCR tests, as well as give rise to unnecessary panic, anxiety, work disabilities, school quarantines, etc.
~ However: this risk is largely offset by the additional special 'confirmatory tests' that are included with each batch of standard tests, and that reduce the probability of 'false positive' test results (after a double saliva test) to less than 1/1000 (~ <0.1%).
risk of unexpected escalations and / or other butterfly' or 'bullwhip' effects as a result of some technical details that currently still need to be - at long last - clarified (and preferably as soon as possible), because otherwise they could cause confusion / disinformation with the users of the respective tests, as they will be marketed by different manufacturers. Obviously, what we are dealing with here are simple screening paper-strip tests and not diagnostic devices, but nevertheless there exists a risk for some (admittedly technically-scientifically perfectly explainable) differences in the field of test criteria (specs / specifications) as used by the different Ag saliva test manufacturers; which could indirectly lead to confusion and / or misplaced dissatisfaction among test users, a phenomenon that should therefore be avoided as much as possible.
After all, there is a real possibility of:
(a) divergent test results of scientific samples, (partially due to :)
(b) divergent quantitative and qualitative benchmark and threshold specifications as used by the various saliva test producers. On this very issue, some notable suggestions were launched in recent weeks (among others by certain academic circles in the US and in Berlin), but today the transparency needed to make rapid progress in this field is still lacking.
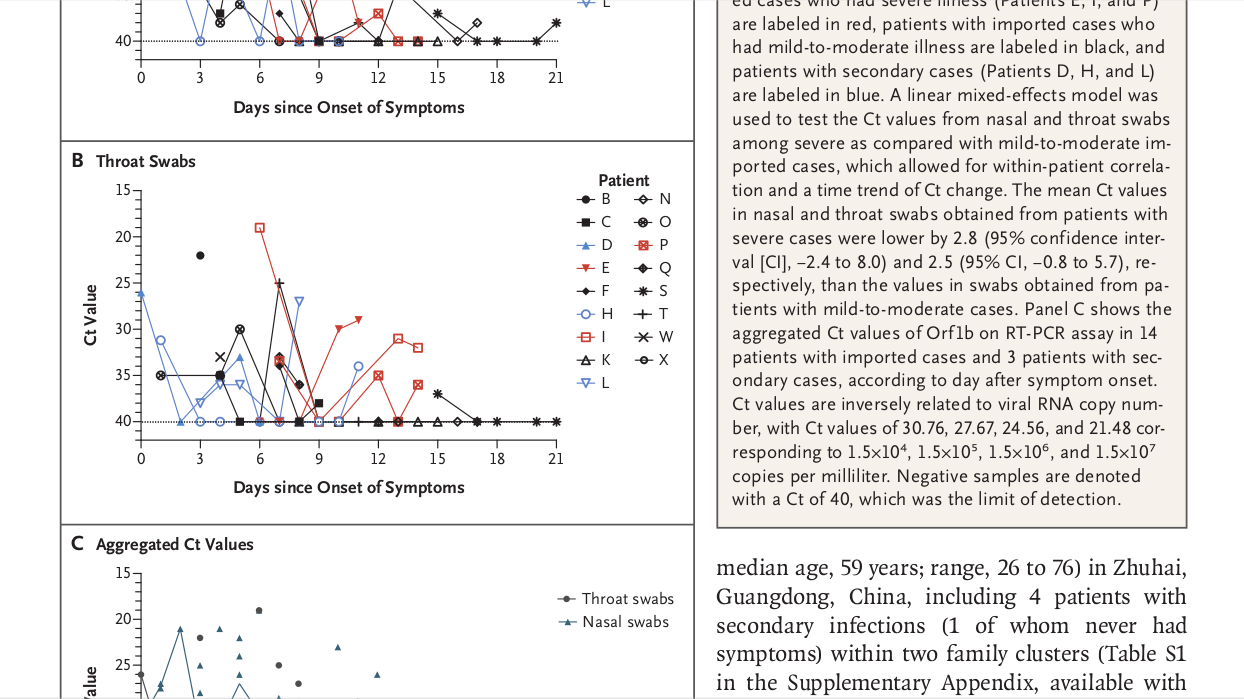
This concerns, for example, the criteria (to be applied) for 'viral loads & shedding' / 'RT-PCR-ct cycle threshold equivalents'; and this both in terms of the relevant ct values and the VL / ct calibration methods. These are important in delineating what actually constitutes a "positive" and what actually constitutes a "negative" saliva test.
In addition, there is a real possibility that the various saliva test producers apply different criteria with regard to the exact method/protocol to be followed by the individual private users for administering the saliva test; among other things each depending on possibly divergent test specifications (e.g. as a result of differences in the molecular composition of the actual antigenic test strips, which may or may not be open source), in function of diverging views on quality control, in function of user support 'at the point of use', etc.
~
However, this mainly concerns scientific-philosophical discussions. Those can quickly (and easily) find a technical / economic / administrative solution: within the acceptable safety margins and within the probability intervals for screening tests; especially in the framework of the pandemic emergency situation Europe finds itself in. Moreover, the quasi-100% reliability of the saliva tests at the time of a so-called 'viral peak' (i.e. the period of 60-72 hours with the highest risk of infection) must also be considered as a key success driver for the lowcost antigen tests. Hence, possibly divergent criteria and, later on, the risk of divergent tests-results between the different saliva test platforms - in case of a virus-positive test - are actually statistically irrelevant (and therefore practically negligible from an epidemiological point of view); whereby it can not or may not be expected that each test user would (wish to) take these differences into account on his/her individual level. Nevertheless one should caution against a cacophony of differing expert opinions or differences in diagnostic interpretations, which may lead to the test users losing confidence or becoming confused and disinformed. In any case, it would be intellectually dishonest for certain public authorities and / or certain academic bodies and / or certain big-pharma companies to abuse this kind of backbench discussions to block the necessary transition to the new screening test-regime. Such hesitations simply amount to culpable negligence on the part of those responsible. After all, what we are dealing with here are (by definition slightly less accurate) mass public health surveillance screening tests, and not (by definition highly accurate) clinical diagnostic tests. This is precisely the crux of the story, and one should therefore refrain from confusing the population / citizens / test users about the tradeoffs at hand ...
limited risk of technical problems and teething problems, whether or not in combination with incorrect use and / or incorrect interpretation of the confirmatory tests supplied with each batch of standard tests, and whether or not organized by 'test-organizing' organizations. This is all the more so, because the 'viral cell load' of a simple saliva sample can be lower than an equivalent nasopharyngeal swab, possibly leading some to conclude 'that opportunities or signals are being missed'
~ However, these risks can be managed to a significant degree, by way of a phased-in deployment of this new low-tech testing technology, by way of preliminary testing and simulations, by way of sampling and quality control, by way of appropriate training and by way of a Europe-wide awareness-raising campaign that is aimed at the individual testers, at the organizing organizations, as well as at some of the health care personnel. Speed and ease of use are precisely the drivers required for widespread public support for these antigen auto-tests as they will underpin their massive, frequent use, eventhough they are less reliable to begin with. After all: one should not put the cart before the horse; and what clearly prevails here is that the European population continues to frequently test itself in massive numbers, without quitting or giving up because of all kinds of discomforts or inconveniences. What counts is that the decentralized population screening and public health surveillance programs can continue unabated. In other words, and as strange as this may sound: in the case of the modern Ag SARS-CoV-2 saliva tests (and this is particularly true from an epidemiological point of view) the ease of use and the fast turnaround times prevail over the accuracy of the test, which comes in second place. Obviously, one must continue to take as much care as possible (or as useful) to avoid testing incidents and testing accidents, yet especially the speed, the massive numbers and the high frequency, but also the low cost and the comparative ease of use, should prevail over the fact that these Ag saliva tests are somewhat less accurate than the gold standard RT-PCR tests.
limited risk of dangerous behavior and / or a careless attitude in some who think that - in the case of a negative, ie "OK" or "GO" test result - they can let go and start taking unnecessary risks: both in the context of social distancing and personal prevention measures, and in the context of the testing strategy; e.g. in case they no longer regularly observe the frequency and the user instructions such as they apply for the respective saliva test regimens.
~ However, once again, an appropriate enforcement policy, in combination with a Europe-wide awareness-raising campaign, can work miracles, especially among certain population groups (e.g. among children, among the elderly, among tourists, among university students, among the homeless, among refugees, among drug addicts. or also: in the case of schools, associations, airlines, bus companies, organizers of sporting events, etc.). In addition, past experience with other home tests (pregnancy tests, HIV tests, etc.) in developed countries such as the EU member states demonstrates that this kind of risks is certainly manageable, and that it is possible to rely on the common sense and civic spirit of our fellow Europeans.







 - WHO Update (3 August 2020).png)








- -
For instance, an RT-PCR test (total cost: up to 100 €) will sometimes turn out a positive result, up to many weeks after the original symptomatic SARS-CoV-2 virus infection, i.e. at a time when the tested individual has probably not been contagious for weeks, because RT-PCR testing can sometimes still detect 'ineffective' genetic virus RNA fragments, which - given the typical 'gold standard' high specificity and particularly (in casu:) the 'gold standard' high sensitivity of the RT-PCR test - will often lead to a misleading 'positive result', and thus also might lead to all kinds of (misplaced) anxiety, discomfort and inconvenience for the tested person and his/her environment.
example (1):
the case where a former COVID-19 patient relying on the diagnostic RT-PCR test (cost: 100 €) still tests positive 7 weeks after disappearance of the disease symptoms, (long) after having ceased being virus contagious, and thus without being able to transfer the virus to people in his / her environment. In a case like this, the RT-PCR test will give a "false true positive" result (since - in some cases - RNA fragments from a fragmented corona virion can still be detected by the RT-PCR many weeks after the initial COVID-19 disease), while a modern antigen paperstrip saliva test (cost: 1 €) would - ceteris paribus - simply test "truly true negative" for SARS-CoV-2-tranmissibility. Evidently, the latter situation offers a much more useful / soothing answer to the test users concerned - while this antigenic paper strip self-test platform is much cheaper, convenient and faster, to start with.
- -
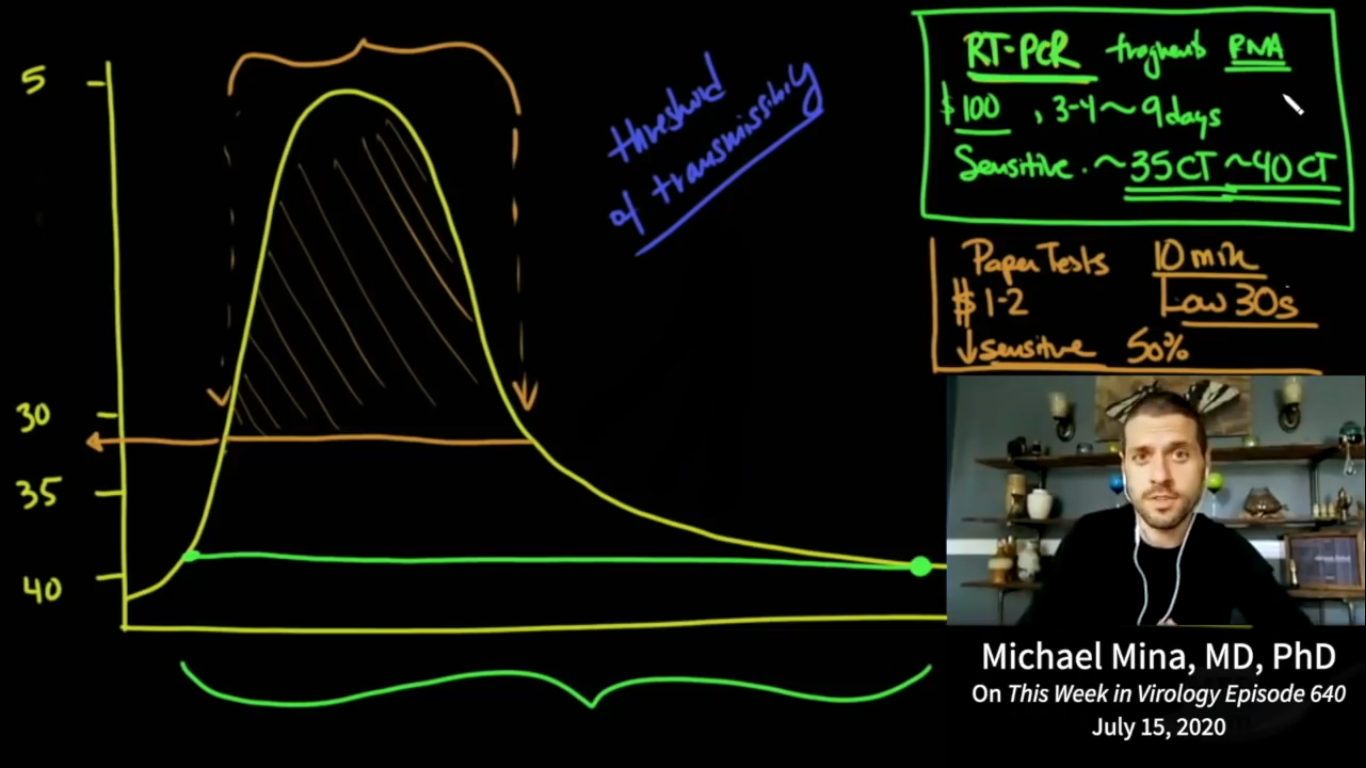
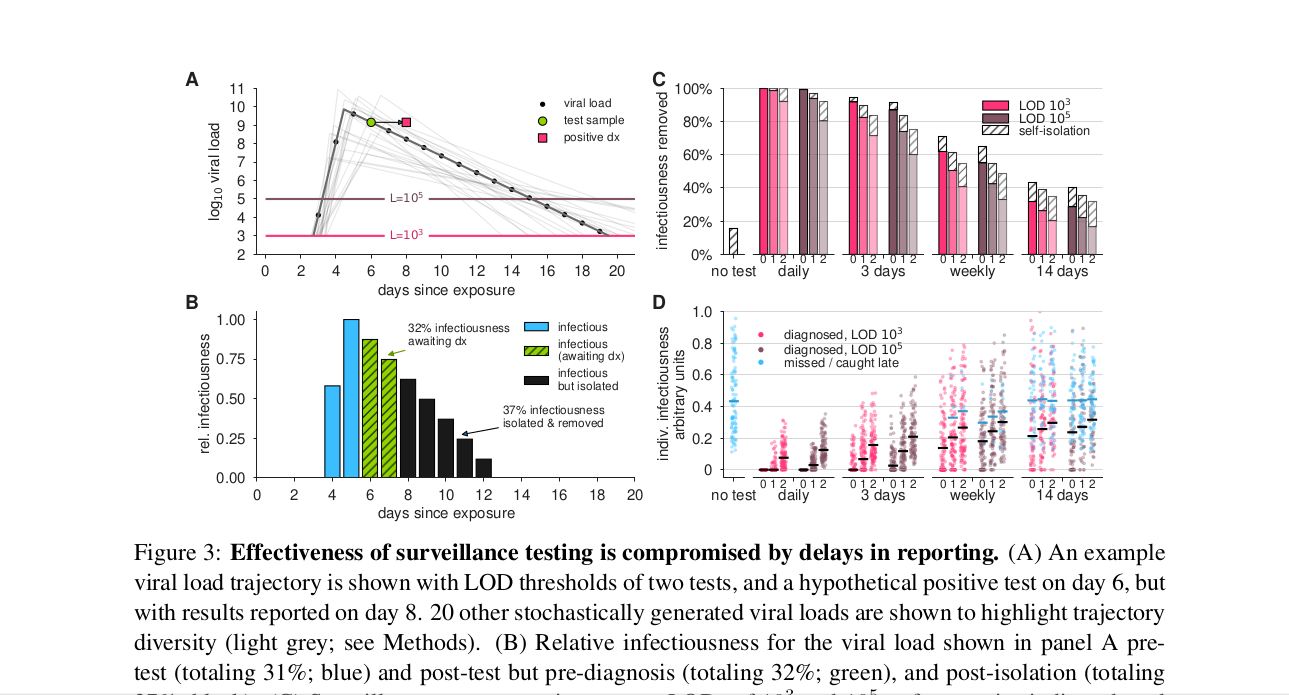
For instance, taking an RT-PCR test (cost: 100 €) can be very time consuming, forcing the test user having to deal with very long waiting lists, queues, testing times, protocols and response times (the so-called total 'turnaround times'), so that it can take an unreasonably long turnaround time before one obtains the test result. Yes, even to the extent that the RT-PCR turnaround times are sometimes so long that the tested individual may long since have been at the origin of further contagion in his/her personal environment. Again, a modern antigenic paper-strip saliva test (cost: 1 €) - ceteris paribus - is likely to give the test-user a compelling "NOT OK" / "NO GO" test result within 15 minutes (not accounting for another 15 minutes for an additional confirmatory test in case the first test is positive indeed), giving the self-test user the opportunity to become immediately aware of the real risk of contamination posed by him/her and of the absolute need for immediate self-isolation. From this point of view, in these concrete circumstances, the antigenic saliva self-test-user and his/her environment are objectively-statistically consisiderably better (safer) off. The availability of much faster (and also much cheaper and easier-to-use) tests, characterised by their almost immediate 'instant' turnaround times, should also allow and motivate large swaths of the population to carry out their own tests massively and frequently (e.g. on a daily basis), thus being one of the most important success factors for this new 'public health' testing strategy. See also Mina et al.: 'Test sensitivity is secondary to frequency and turnaround time for COVID-19 surveillance' (medRxiv preprint doi: https://doi.org/10.1101/2020.06.22.20136309, September 8, 2020).
example (2):
the case of a nasal swab RT-PCR test administered in a hospital: this test is administered by specialized staff in the hospital, before being analysed according to a time-consuming protocol/procedure that is handled with highly specialized equipment operated by highly trained para-medical personnel; with a total reporting and response time back to the tested clinical 'patient' that is all-too-often exceeding 24 hours. Such diagnostic laboratory tests are - in any case - relatively expensive, with an estimated total cost (even without internalizing every external cost) of more than € 100 per test; instead of less than 1 € for a paper strip saliva test.
- -
MACRO-testing ~ 1€ paper strip tests ~ COVID-19-public-health-surveillance ~ 'Quick & Dirty' ~ European population screening ~ the 'SCREENING method':
This public mass screening method mainly focuses on the 'social demonstration' of "Corona test NEGATIVITY": this testing-strategy relies on the individual test users themselves to carry out the tests easily, quickly and cheaply. After all, all is needed is for the individual users to administer the paper-strip tests themselves (cost: approximately € 1 per test). This test method can also be used in an 'organized' way by organizing institutions.
example:
the case of a school: a daily paper strip self-test of all students and of all staff members (estimated cost: less than 1 € per test) can be done before leaving home in the morning, or otherwise immediately upon arrival at school. Indeed, the individual users (or their parents) would each find out the 'GO' / 'NO GO' or 'OK' / 'NOT OK' result on the paper strip within 15 minutes after taking their self-test.
An additional argument for this so-called 'COVID-19 surveillance' method is the private, anonymous nature of the antigenic 'disposable' saliva tests: in principle, each user takes the test on his/her own - at their own initiative and with respect of their personal privacy. In other words, this decentralized anonymous public health 'surveillance' is based on the so-called auto-screening principle (in reality this comes down to an epidemiological population survey). Therefore it should certainly not be confused with other (digitized) forms of 'digital surveillance state' aspects of our modern European healthcare, some of which - as became apparent in the course of the ongoing corona pandemic - are all too often lurking around the corner: telephone appointments, telephone consults (whether or not based on video conference calls), electronic 'track & trace' guest lists, corona apps with geo-location and / or bluetooth recognition, electronic patient files, robotized invoice processing, automatic data exchange between institutions and labs, cloud computing, artificial intelligence, digital outsourcing, data mining, etc. All of which is - by definition - completely out of the question here,.. since everything is still - literally - settled on paper.
- -
MICRO-testing ~ 100€ laboratory tests ~ SARS-CoV-2 detection ~ 'Lean & Clean' ~ useful for scientific or medical research ~ the 'DIAGNOSTIC method':
This private diagnostic laboratory detection method focuses mainly on the medical demonstration of 'Corona test POSITIVITY': one will be able to rely on very precise, very accurate (highly-sensitive / highly-specific) clinical technology that is typically used in hospitals or in clinical laboratories, using capital-, labor- and time-intensive equipment, protocols and reagents (total cost: approx. € 100 per test). This test method is not only expensive, but also inherently slow and cumbersome; and it is therefore difficult to use in an 'organized' way, which means that it will usually be taken on an individual basis.
example:
the case of a so-called 'testing street with Martians in PPE': a professional basketball player came back from vacation 2 weeks ago, participated in a meeting with the coaching staff 1 week ago, and in the meantime found out that some of the fellow guests at his vacation-hotel on their return home were showing COVID-19 symptoms. The basketball player has never fallen ill himself, but the club management wants to make 100% sure (also in order to protect the coaching staff) whether the athlete in the meantime became infected (albeit asymptomatically), and whether the athlete himself could possibly also have posed and/or still poses an infection risk for his immediate enviroment. This can - in this specific case - be verified very precisely by means of an RT-PCR test carried out on all those involved; while the individual 'infectiousness' of each of them could easily be screened for by means of a do-it-yourself saliva test - e.g. in an 'organized' setting: every day in the morning and in the afternoon, at the beginning of each basketball training session.